Evidence shows that lowering blood pressure (BP) decreases the risk of adverse cardiovascular outcomes such as heart disease, stroke, and death.1-6 It may also slow the progression of kidney damage when used by people with chronic kidney disease (CKD).7 Further, meta-analyses as well as national and international guidelines suggest that lowering BP decreases risk of these outcomes regardless of which agent is used.1-5,8
Angiotensin receptor blockers (ARBs) are a first-line treatment for all stages of hypertension as a monotherapy or in combination with one or more other antihypertensive agents.3,6 Studies have found no significant efficacy differences between the individual ARBs.9
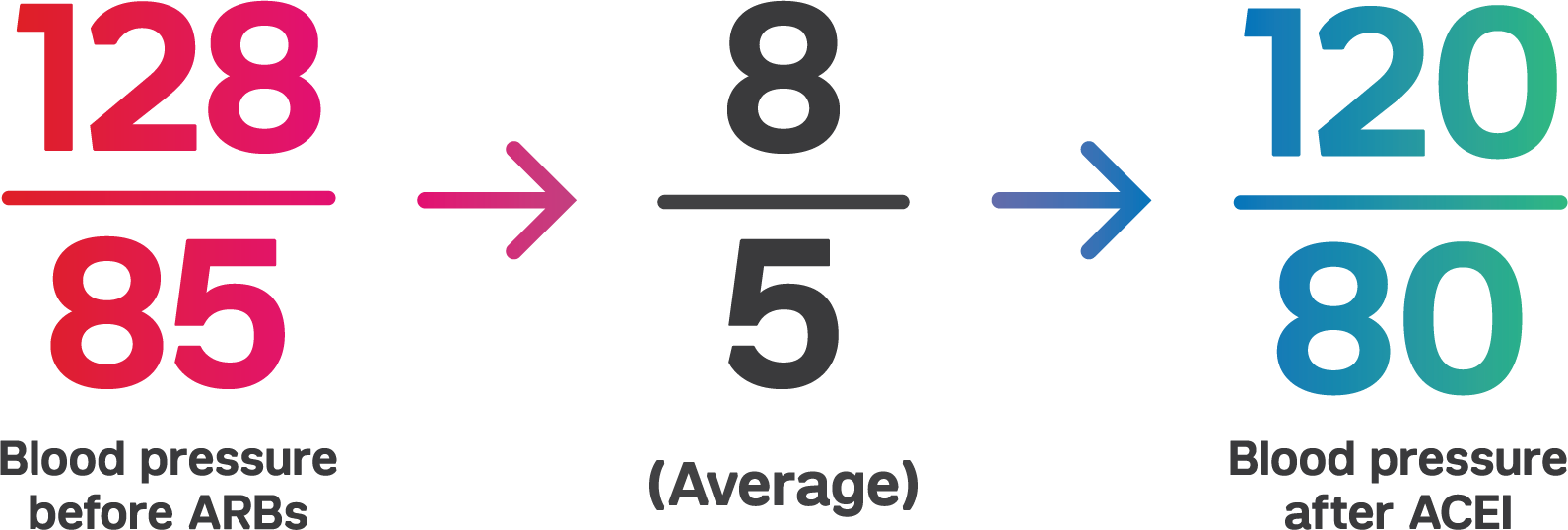
Monotherapy trials show the BP lowering efficacy of ARBs.10-13 A 2008 Cochrane Review meta-analysis found 46 randomized controlled trials of 9 ARBs (n=13,451).9 It looked at the antihypertensive efficacy of the ARBs on dose-related trough BP.9 The baseline BP was 156/101 mm Hg across the trials. ARBs lowered BP measured 1 to 12 hours after the dose by about 12/7 mm Hg. The best estimate of trough BP lowering effect for ARBs based on the largest trials was -8 mm Hg for systolic blood pressure and -5 mm Hg for diastolic blood pressure. The analysis also found that a dose of 50% of the maximum (max) daily dose had a BP lowering effect that was 80% of max and that ARB doses above the max dose did not lower BP significantly any more than the max dose.
A 2014 meta-analysis compared the antihypertensive efficacy of the most common ARBs used as hypertension monotherapy compared to the ARB losartan evaluated by 24-hour ambulatory blood pressure monitoring (ABP).10 The study found a shallow dose-response curve with a BP decrease of 10.3/6.7 (systolic/diastolic), 11.7/7.6, and 13.0/8.3 mm Hg s at 25% of the max dose, 50% max dose, and with the max dose of all ARBs respectively. Analyses showed the ARB losartan lowered blood pressure less at all doses compared to other ARBs. Losartan at a 50 mg dose lowered ABP less than other ARBs at 50% max dose by 2.5 mm Hg systolic (p<0.0001) and 1.8 mm Hg diastolic (p=0.0003). Losartan at a 100 mg dose lowered ABP less than other ARBs at a max dose by 3.9 mm Hg systolic (p=0.0002) and 2.2 mm Hg diastolic (p=0.002).
Progression of kidney disease may be slowed by ARBs.7 The 2012 KDIGO clinical practice guideline recommends an ARB or an angiotensin converting enzyme inhibitor (ACEI) be used in diabetic adults with CKD and urine albumin excretion 30 to 300 mg/24 hours. The guideline also recommends that an ARB or ACEI be used in both diabetic and non-diabetic adults with CKD and urine albumin excretion >300 mg/24 hours.
References
- Abraham HMA, White CM, White WB. The comparative efficacy and safety of the angiotensin receptor blockers in the management of hypertension and other cardiovascular diseases. Drug Saf 2015; 38 (1): 33-54.
- Ahluwalia M, Bangalore S. Management of hypertension in 2017: targets and therapies. Curr Opin Cardiol 2017; 32 (4): 413-421.
- James PA, Oparil S, Carter BL, et al. 2014 evidence-based guideline for the management of high blood pressure in adults. JAMA 2014; 311 (5): 507-520.
- Pignone M, Viera AJ. Blood pressure treatment targets in adults aged 60 years or older. Ann Intern Med 2017; 166 (6): 445-445.
- Qaseem A, Wilt TJ, Rich R, Humphrey LL, Frost J, Forciea MA. Pharmacologic treatment of hypertension in adults aged 60 years or older to higher versus lower blood pressure targets: a clinical practice guideline from the American College of Physicians and the American Academy of Family Physicians. Ann Intern Med 2017; 166 (6): 430-430.
- Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a reportof the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2017.
- KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl (2011) 2013; 3 (1): i-150.
- Bangalore S, Fakheri R, Toklu B, Ogedegbe G, Weintraub H, Messerli FH. Angiotensin-converting enzyme inhibitors or angiotensin receptor blockers in patients without heart failure? Insights from 254,301 patients from randomized trials. Mayo Clin Proc 2016; 91 (1): 51-60.
- Heran BS, Wong MM, Heran IK, Wright JM. Blood pressure lowering efficacy of angiotensin receptor blockers for primary hypertension. Cochrane Database Syst Rev 2008; (4): Cd003822.
- Makani H, Bangalore S, Supariwala A, Romero J, Argulian E, Messerli FH. Antihypertensive efficacy of angiotensin receptor blockers as monotherapy as evaluated by ambulatory blood pressure monitoring: a meta-analysis. European Heart Journal 2014; 35 (26): 1732-1742.
- Oparil S, Williams D, Chrysant SG, Marbury TC, Neutel J. Comparative efficacy of olmesartan, losartan, valsartan, and irbesartan in the control of essential hypertension. J Clin Hypertens (Greenwich) 2001; 3 (5): 283-291, 318.
- Pfeffer MA, Swedberg K, Granger CB, et al. Effects of candesartan on mortality and morbidity in patients with chronic heart failure: the CHARM-Overall programme. Lancet 2003; 362 (9386): 759-766.
- Timmermans PB, Duncia JV, Carini DJ, et al. Discovery of losartan, the first angiotensin II receptor antagonist. J Hum Hypertens 1995; 9 Suppl 5: S3-18.
.png)
